Introduction
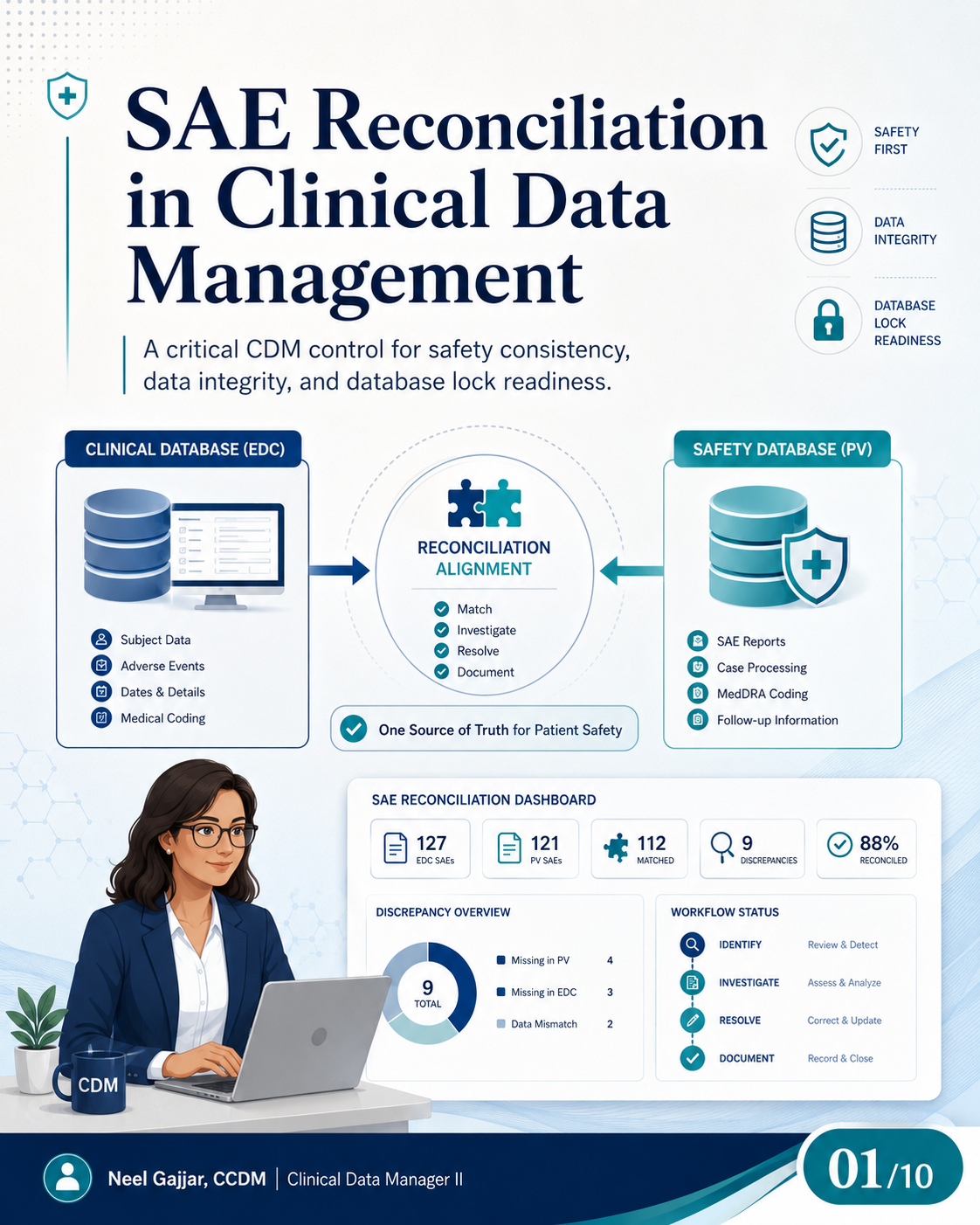
SAE reconciliation is one of the highest-stakes activities in clinical data management. A single unreconciled Serious Adverse Event - existing in the EDC but not in the safety/PV database, or carrying different dates, terms, or seriousness criteria across systems - is a patient safety risk, a regulatory inspection risk, and a database lock risk.
SAE reconciliation supports patient safety, reliable study data, and database lock readiness.
Why SAE Reconciliation Matters
The EDC and the Safety/PV database both hold the same safety event - but they hold it separately. Each system captures a different operational view of the same clinical reality. Both must agree.
EDC holds: Subject data, AE pages (onset, resolution, severity), dates, and MedDRA coding applied to AE records.
Safety Database (PV) holds: SAE reports, case processing, MedDRA coding applied by the safety team, follow-up information, and regulatory reporting records.
Five risks from unreconciled SAE data:
- Incomplete safety visibility - Key risks may be missed or underreported if events are not captured consistently across both systems
- Inconsistent reporting - Discrepancies create inconsistencies across safety submissions, annual safety reports, and expedited reports
- Inspection findings - Regulatory inspectors compare EDC records with the safety database as a standard inspection activity
- Delayed database lock - Unresolved SAE discrepancies block the safety review and delay lock
- Reduced confidence in study data - Stakeholder trust is undermined when the safety story cannot be verified across systems
SAE reconciliation confirms that clinical and safety records remain complete, consistent, and traceable across study systems.
Where SAE Data May Exist
One safety event may appear across six sources:
- EDC / Clinical Database - AE/SAE pages, onset and resolution dates, severity, seriousness criteria, action taken, and relationship to study drug
- Safety Database / PV System - Case intake, case processing, medical review, MedDRA coding, narrative, regulatory reporting status, and follow-up management
- Medical Review / Coding Outputs - MedDRA term comparisons and query outputs from the coding team; terms applied in EDC and PV must be consistent and version-aligned
- Hospital or Source Records - Discharge notes and medical records with primary source information for hospitalisation dates, diagnoses, and outcomes
- Vendor or External Data - Central lab results or ECG findings relevant to seriousness or causality assessment
- Narratives and Listings - Safety listings and cross-check reports that should reflect a reconciled source
Key Fields to Reconcile
| Field | Reconciliation Standard |
|---|---|
| Subject ID | Correct patient in both systems; format must be consistent |
| Event Term / Description | Same medical event meaning; MedDRA PT alignment across EDC and PV |
| Start Date | Aligned onset date between EDC site record and PV case |
| End or Resolution Date | Closure date aligned between systems |
| Seriousness Criteria | Hospitalization, death, life-threatening, medically important event - same classification in both |
| Outcome / Current Status | Recovered, ongoing, fatal, or unknown - consistent across systems |
| Causality / Relationship | Related or not related - consistent with investigator assessment |
| Severity / Grade | Compare when collected and applicable |
Common SAE Reconciliation Discrepancy Types
- Present in one system only - An SAE not in the PV database is unreported from a pharmacovigilance perspective - the highest-risk discrepancy type
- Date mismatch - Under ICH E2A, expedited safety reports (7-day for fatal/life-threatening, 15-day for other unexpected serious events) are calculated from the day the sponsor first receives information. If the onset date in PV does not match the EDC, the reporting timeline may be wrong - a potential regulatory violation. Treat date discrepancies as high priority
- Event term mismatch - MedDRA PT alignment between EDC and PV is required; the same event must be coded to the same or equivalent PT. PT discrepancies affect signal detection and safety tables. Both systems should use the same locked MedDRA version as defined in the DMP or SAP
- Seriousness criteria mismatch - An event classified as serious in the EDC but not in PV is a regulatory reporting risk
- Outcome mismatch - Patient outcome status used in narratives and submissions must be consistent between systems
- Causality mismatch - The investigator's causality assessment in the EDC should match the PV record; discrepancies require medical review
- Missing hospitalisation details - Hospitalization is a seriousness criterion; incomplete hospitalisation data creates a gap in the safety record
- Incomplete follow-up information - Outstanding follow-up creates open SAE cases that cannot be closed before lock
The SAE Reconciliation Process: Six Steps
- Receive Data - Extract safety data from both EDC and PV; confirm the extract is current, complete, and covers the same scope
- Compare Records - Match subject records across systems using predefined matching rules; flag every unconfirmed match
- Identify Discrepancies - Detect missing records, conflicting field values, or inconsistent classifications; categorise by type and severity
- Investigate with Teams - Collaborate with Safety/PV and sites; CDM owns clinical data accuracy, Safety/PV owns database accuracy; do not resolve unilaterally
- Resolve and Update - Correct data in the appropriate system based on the verified source; document which system was updated and why
- Document and Close - Record actions taken, rationale, and links to supporting documents; retain audit trail; re-run the reconciliation check to validate resolution
Roles and Ownership
| Role | Responsibilities |
|---|---|
| CDM | Review clinical records in EDC; track discrepancies; support closure; own data accuracy and reconciliation quality |
| Safety / PV | Confirm safety details in PV database; ensure follow-up is complete; provide safety expertise and oversight |
| Medical / Clinical Team | Clarify clinical context; review outcomes; provide medical judgement on causality and seriousness |
| Programming / Vendor Support | Provide reconciliation extracts; support mappings and technical alignment; investigate system-level issues |
Clear ownership for every discrepancy accelerates resolution and prevents items from remaining open without a responsible party.
Practical Discrepancy Workflow: Detection to Closure
- Discrepancy detected - Mismatch identified during routine reconciliation
- Verify source records - Check original site record, EDC audit trail, and PV case history before raising a formal item
- Raise reconciliation item - Subject ID, event, field in question, value in EDC, value in PV, and supporting evidence
- Query or discuss if needed - Site query, Safety/PV discussion, or source document review to obtain additional information
- Update the correct system - Based on the verified source; document which system was updated and why
- Document the resolution - Actions taken, rationale, and links to supporting documents
- Close the item - Confirm in the reconciliation tracker; validate in the output; ensure fully resolved before marking closed
Risks of Weak SAE Reconciliation
Five downstream impacts:
- Incomplete safety profile - Key safety risks missed or underreported
- Inconsistent reporting - Discrepancies across regulatory submissions, DSURs, and IND annual reports
- Delayed database lock - Unresolved SAE discrepancies block the lock readiness check
- Audit or inspection findings - Regulatory inspectors citing EDC-to-PV inconsistencies as findings
- Reduced confidence in study data - Stakeholder trust undermined when clinical and safety records cannot be verified as consistent
Weak reconciliation does not just create discrepancies - it reduces confidence in the reliability of the safety story.
Final Takeaway
- Start early - Integrate reconciliation planning into study start-up and database build; define process, matching fields, and ownership before the first SAE is reported
- Compare consistently - Use standardised queries and alignment logic to ensure consistent, repeatable comparisons across every cycle
- Document clearly - Maintain clear evidence, rationale, and audit trails for every reconciliation activity
- Resolve proactively - Do not allow SAE discrepancies to age; SAE reconciliation completion with formal sign-off is a documented database lock prerequisite
In blinded clinical trials, the PV database may contain unblinded treatment information. CDMs who are blinded must follow blinding control procedures when accessing or reconciling SAE data. Accessing treatment-identifying information without authorisation is a protocol deviation and a blinding breach.
This content is AI-assisted and expert-reviewed. All regulatory references are verified against ICH GCP E6(R2), ICH E2A, ICH E2B, FDA 21 CFR Part 312, and applicable clinical data management standards. Content is intended for clinical research professionals for educational and professional development purposes.
About the Author
Neel Gajjar
CCDM®Clinical Data Manager II
Clinical Data Manager specialising in EDC systems, CDISC standards, and GCP-compliant data governance. Creator of the Clinical Research Learning Hub — a platform built to make rigorous clinical research education accessible to every professional in the field.
Connect on LinkedInAll content is expert-written and SME-reviewed. Regulatory references are verified against current ICH GCP E6(R2), FDA, and EMA guidance.
Comments
Leave a comment