Introduction
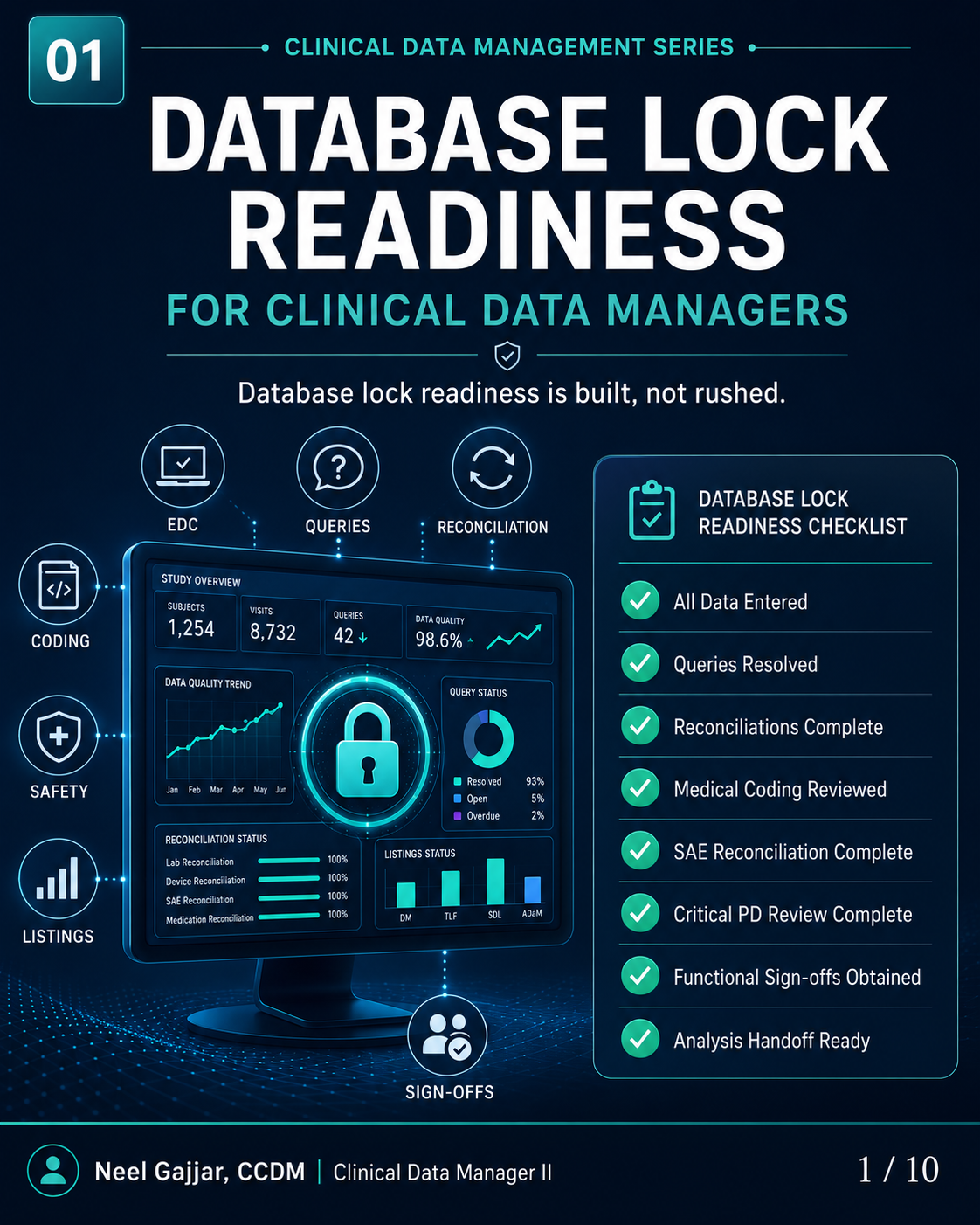
Database lock readiness is built, not rushed. It is one of the most consequential milestones in a clinical trial - the point at which all data entry, query resolution, reconciliation, coding, and review must be complete, documented, and signed off before the dataset is frozen for statistical analysis.
All lock readiness criteria, roles, and sign-off requirements should be defined in the Data Management Plan (DMP) before the study begins. The DMP is the reference document for the lock process - not improvised at the lock meeting.
Many organisations operate a two-stage lock: a soft lock (data entry frozen, CDM review complete, queries dispositioned) followed by a hard lock (full functional sign-off obtained, analysis transfer authorised). Both stages require documented readiness evidence.
Database Lock is Not a One-Day Activity
Readiness is built across the full study lifecycle through five phases:
Study Setup - Define structures, standards, and validation rules early
Data Collection - Capture accurate data with real-time edit checks and consistency validation
Data Review - Review, query, and resolve to ensure complete and reliable data
Freeze - Review data and prepare for final reconciliation activities
Database Lock - Confirm readiness, obtain approvals, and lock the database
Key message: A smooth lock happens when setup, review, reconciliation, and sign-offs are controlled before the final lock meeting - not managed reactively during it.
Lock Readiness Starts at Study Setup
Six setup elements directly determine how difficult or smooth the database lock will be:
Clean eCRF Design - Collect the right data in the right place; every field must have a clear purpose and downstream SDTM mapping
Edit Check Logic - Catch issues early without overburdening sites; target protocol-critical relationships, not noise
Data Review Rules - Define what must be reviewed and by whom; document this in the DMP before study start
Vendor Planning - Plan transfers, ownership, and timing for all external data streams before first patient enrolled
Reconciliation Expectations - Set matching rules before the first transfer; define acceptable tolerances and escalation paths
Role Alignment - Clarify responsibilities across DM, clinical operations, biostatistics, medical coding, safety, and vendor/sponsor
Better setup = fewer surprises at freeze and lock.
Data Entry Completeness
Before lock, expected data must be entered, explained, or documented. Four criteria define completeness:
All expected forms entered - Required forms are present for each subject and visit
Missing pages identified - Outstanding gaps are visible and tracked with an owner and resolution status
Not-done status documented - Protocol-required assessments not performed are marked with applicable reason, not left blank
Outstanding gaps documented and reviewed - Remaining gaps are justified per study process and formally accepted as part of the lock package
Completeness is a lock-readiness control, not a statistical metric.
Open Queries and Acceptable Exceptions
A query response is not enough - it must be reviewed and dispositioned. Every open query at lock must have one of four statuses:
Resolved - Issue corrected and ready to close
Answered and Reviewed - Response assessed and accepted by CDM
Documented Exception - Justified and accepted per study process with documented rationale
Escalated - Lock-impacting or recurring issue raised for action before the lock meeting
CDM Check: Before freeze or lock, each open item should have a clear status, owner, and next step. A query without a disposition is a lock blocker.
External Data and Reconciliation
Vendor and external data must be complete, current, and reconciled. External data streams requiring reconciliation include:
Central Lab - lab results and reference values
ePRO/eCOA - patient-reported outcomes and electronic assessments
ECG - cardiac waveform data and reports
IRT - randomisation and drug supply data (IRT reconciliation includes matching randomisation records, drug dispensing records, and IP accountability documentation - any discrepancy here is safety-critical and must be resolved before lock)
Safety/PV - AE/SAE and safety information from pharmacovigilance systems
Lock-ready data criteria: Final transfers received · Reconciliations complete · Discrepancies resolved · Evidence documented.
Other Critical Readiness Areas
Medical Coding
AEs, concomitant medications, and medical history must be coded per the applicable dictionary (MedDRA, WHO Drug) and reviewed for completeness and consistency. The MedDRA and WHO Drug dictionary versions used must be documented and locked - recoding after database lock due to a dictionary version change is a significant and avoidable rework event.
SAE Reconciliation
All SAEs in the EDC must be matched against the safety/PV database. Discrepancies in onset date, seriousness criteria, outcome, or narrative must be reviewed and resolved before lock.
Protocol Deviations
Critical deviations must be reviewed, categorised, and documented in the listings before freeze.
Final Listings Review
Trends, outliers, and missing data must be reviewed before freeze - not during the lock window.
Functional Sign-Offs
Database lock requires formal sign-off from each function with a stake in data quality:
Data Management - all CDM readiness criteria met
Clinical Operations - site data complete, queries resolved
Medical Coding - coding complete and reviewed
Biostatistics - ready for analysis transfer
Safety - SAE reconciliation complete
Vendor/Sponsor - external data transfers and reconciliation finalised
Sign-off is an attestation, not a formality. Every sign-off must be captured in the TMF or equivalent study record.
Practical Lock Readiness Checklist
Readiness AreaStatusData entry completenessCompleteOpen queriesComplete / In progressExternal data transfersIn progressReconciliation closureIn progressMedical coding reviewCompleteSAE reconciliationIn progressProtocol deviation reviewCompleteFunctional sign-offsPending
Items still marked Pending or In progress at the lock meeting are lock blockers - they must be resolved, accepted as documented exceptions, or formally escalated before the lock proceeds.
Final Takeaway
Database lock readiness is built, not rushed.
A strong lock is the result of good planning, consistent review, and documented control throughout the study.
A well-executed database lock produces a dataset that is:
Complete - all expected data entered, explained, or documented
Reviewed - all data through the appropriate review process
Documented - all exceptions, deviations, and reconciliation decisions on record
Reconciled - all external data streams matched and verified
Ready for analysis - the dataset moves directly to statistical programming without further cleaning
About the Author
Neel Gajjar
CCDM®Clinical Data Manager II
Clinical Data Manager specialising in EDC systems, CDISC standards, and GCP-compliant data governance. Creator of the Clinical Research Learning Hub — a platform built to make rigorous clinical research education accessible to every professional in the field.
Connect on LinkedInAll content is expert-written and SME-reviewed. Regulatory references are verified against current ICH GCP E6(R2), FDA, and EMA guidance.
Comments
Leave a comment