Introduction
Artificial intelligence is no longer a concept on the horizon for Clinical Data Management - it is already reshaping how CDM teams work across every stage of the clinical data lifecycle. But using AI effectively requires strategy, not experimentation. The question is not whether to adopt AI, but where it adds the most value and how to govern it so adoption remains inspection-safe.
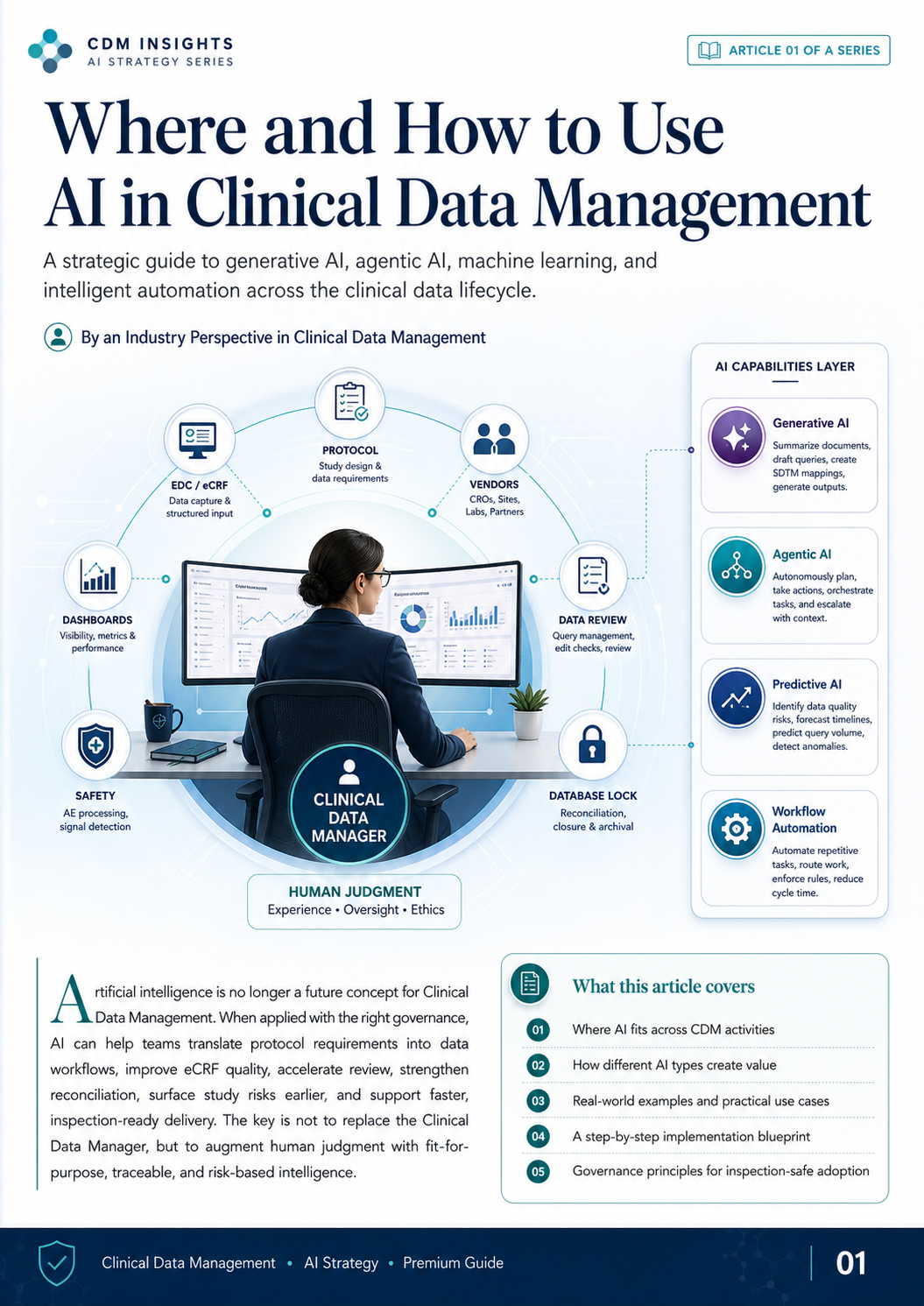
This guide covers four AI capability layers relevant to CDM - Generative AI, Agentic AI, Predictive AI, and Workflow Automation - mapped to real CDM activities, with a phased implementation plan and a governance model grounded in GCP principles.
1. The AI Opportunity Across the CDM Lifecycle
Clinical Data Management is a controlled delivery pathway. It starts with protocol interpretation, moves through EDC build, data collection, monitoring, query resolution, reconciliation, and ends at database lock and archival. AI creates value at every stage - but the type of AI matters.
The core principle: use AI as a task-specific copilot, not a blanket solution. The strongest implementations match the right AI capability to the right CDM problem.
Best-fit AI by lifecycle stage:
- Protocol & DMP Phase → Generative AI: drafts first-pass documents, extracts endpoints, identifies gaps against prior studies
- EDC Build & eCRF Review → Generative AI + Predictive AI: generates validation scripts, detects duplicate or missing items
- Data Collection & Monitoring → Agentic AI + Predictive AI: monitors field-level anomalies, triggers issue escalation
- Query Management → Generative AI + Workflow Automation: drafts queries, routes to site, tracks resolution
- Reconciliation → Workflow Automation: compares EDC and vendor files, flags mismatches
- Database Lock → Predictive AI: surfaces outstanding dependencies, consolidates readiness signals
2. Generative AI in Clinical Data Management
Generative AI - large language models capable of reading, interpreting, and producing text - delivers the fastest productivity gains in CDM because so much CDM work is language-based: reading protocols, writing documents, drafting queries, and interpreting standards.
When to use generative AI:
- First draft of protocol-aligned documents (DMP sections, edit check specifications, data review plans)
- Reading dense regulatory or sponsor source documents and producing structured summaries
- Translating requirements into standardised terminology across CDISC, MedDRA, or sponsor conventions
- Drafting and clarifying queries, including site-specific language adaptation
- Standards interpretation: comparing aCRF structures against CDASH/SDTM expectations
When NOT to use generative AI:
- Final medical or regulatory decisions
- Automatically changing clinical data without human verification
- Outputs that feed directly into regulatory submission without CDM review
- Unverified CDISC or regulatory standards interpretations - generative AI can produce plausible-sounding but factually incorrect guidance; always verify against primary source documents before including AI-generated standards text in submission deliverables
Real-World Application Areas
Protocol to Requirements
AI reviews protocol documents, maps out assessments, endpoints, and variables, and highlights critical requirements for data collection. This replaces hours of manual protocol dissection with a structured output for CDM review.
Document Drafting
AI accelerates creation of DMP first-pass sections, CRF annotation notes, and review checklists - consistent with the protocol and aligned to sponsor standards.
Query and Communication Support
AI helps draft clear, site-appropriate queries, categorises by data impact, and can generate standard follow-up emails, reducing per-query cycle time.
Standards Interpretation
AI assists with CDISC mapping by comparing draft aCRF labels against CDASH standards, flagging non-standard naming, and identifying downstream SDTM classification issues.
3. Agentic AI and Workflow Automation
Agentic AI goes beyond content generation - it can coordinate multi-step tasks, monitor conditions, trigger actions, route issues, and escalate based on time, context, and logic. This is where AI compresses manual follow-up and cycle time.
Common CDM agentic workflow use cases:
- Query Follow-Up Orchestration - monitors query status, identifies queries approaching SLA windows, reminds sites, and escalates critical issues
- Vendor Data Intake Control - checks incoming vendor files against expected format, structure, and delivery schedule; alerts on anomalies or missing transfers
- Form Availability Coordination - monitors CRF completion rates by site and visit, surfaces collection gaps before monitoring visits
- Issue Routing - categorises open issues by type, priority, and responsible party; routes to DM, site, or vendor with a documented, inspectable audit trail at every step
- Meeting Preparation - aggregates open query listings, trend summaries, and action items for DM team review meetings
- Lock Readiness Coordination - monitors open queries, outstanding reconciliation items, database lock checklist dependencies, and flags items requiring senior review
Human checkpoint is required before autonomous actions are executed. Agentic AI should trigger, prepare, and surface - not execute unilaterally. Human approval and audit trail documentation remain mandatory under ICH GCP.
4. Predictive AI, Anomaly Detection, and Risk Prioritisation
Predictive AI analyses patterns and signals across the trial database to identify where risk is highest before it becomes an issue. CDM teams using predictive tools can shift from reactive query resolution to proactive risk management.
What predictive AI should do:
- Flag Anomalous Clinical Data - identify values outside physiologically expected ranges, statistically unusual distributions, and isolated inconsistencies across visits
- Query Frequency Forecasting - identify sites or forms trending toward elevated query volumes based on early collection patterns
- Visit Risk Window - surface visits with historically high error rates or protocol deviations, helping monitors prioritise
- Handle Reconciliation Dates - detect delays between EDC entry and vendor file receipt; flag data entry delays against expected timelines
- Data Entry Delay Detection - identify subjects or sites with systematic latency patterns that may signal data quality or site resource issues
- Abnormal Pattern Detection - discover distributions, unexpected consistencies, or outliers that may indicate systemic data quality issues
What predictive AI should NOT do:
- Independently decide that data is wrong
- Replace the medical monitor's or sponsor's safety review judgement on SAE causality or signal escalation - safety decisions remain with qualified medical personnel
- Generate automated database changes without human review and approval
- Serve as the sole determinant for any regulatory or safety escalation decision
A well-implemented risk dashboard provides a composite risk score by site or subject, aggregating signals from query rate, data latency, visit completion, and anomaly detection - giving CDM managers a single view for prioritisation.
5. Real-World CDM Use Cases by Activity
| CDM Activity | AI-Enabled Use Case |
|---|---|
| Protocol Review | Extract assessment data, endpoint data, and operational risks |
| DMP Development | Generate first-pass sections, route work, escalate exceptions |
| eCRF Review | Compare fields against protocol; detect missing or duplicate items |
| Edit Check Review | Identify false-positive risk, missing edge cases, poor wording |
| UAT Planning | Generate positive, negative, and boundary test case scenarios |
| Data Cleaning | Draft clear queries and prioritise by clinical data impact |
| Vendor Reconciliation | Compare EDC against central lab and IRT files; flag missing or mismatched records |
| Risk Review Meetings | Summarise key trends, risks, and action items |
| Site Performance Monitoring | Identify late entry, report unusual deviations, flag quality signals |
| Database Lock Readiness | Consolidate outstanding issues and unresolved dependencies |
The highest-value AI cases are those that save review time, improve consistency, and make risks visible earlier.
Three Illustrative Examples
A. PK Timepoint Review - AI scans scheduled PK windows against collection timestamps and flags samples outside the acceptable window for human review, reducing the time for PK outlier identification from days to minutes.
B. Lab Check - At accession, AI cross-references lab reference ranges against the protocol specification and identifies missing subjects, incremental issues, or values outside expected units.
C. Safety Follow-Up - AI monitors open safety-related queries, summarises resolution status, highlights missing action items, and flags overdue responses for CDM escalation.
6. A Full-Proof Implementation Plan
Phase 1 - Foundation and Governance (Weeks 1–4)
Focus: Define before you deploy.
- Document approved AI use cases and operational boundaries
- Establish governance charter, RAI (Responsible AI) principles, and decision rights
- Set human review checkpoints for all AI-assisted outputs
- Document roles, SOPs, and review checklists
- Identify training data sources and acceptable AI tool list
- Initiate Computer System Validation (CSV) package for each AI platform under GAMP 5 Category 4 or 5 - AI tools used in regulated data environments require their own validation, separate from workflow validation
Key deliverables: AI use registry, governance charter, R&D decision tree, SOPs, CSV plan for each AI platform
Phase 2 - Pilot Use Cases (Weeks 5–16)
Focus: Start with assistive AI, not autonomous AI.
- Select 2–3 high-value, lower-risk use cases (e.g. query drafting, DMP section generation)
- Run parallel outputs - AI draft vs. current process - for calibration
- Define pass/fail criteria before the pilot begins (e.g. ≥30% reduction in query drafting time with no increase in query rejection rate)
- Gather CDM team and site feedback
- Document lessons learned and update governance
Key deliverables: Pilot results, time and quality metrics, lessons learned report
Phase 3 - Workflow Integration (Weeks 17–26)
Focus: Embed AI into standard CDM workflows.
- Connect AI to EDC, trackers, and vendor exchange systems
- Define escalation logic and exception handling
- Validate integrated workflows end-to-end
- Generate an inspection-ready validation package including test scripts, expected vs. actual results, and deviation handling documentation
Key deliverables: Integrated workflows, validation documentation, escalation protocol
Phase 4 - Scale and Continuous Improvement (Weeks 26+)
Focus: Expand and measure.
- Roll out validated workflows to additional trials or therapeutic areas
- Monitor performance and KPIs dashboards
- Conduct quarterly AI performance and risk reviews
- Maintain ongoing governance review
Recommended starting point: Begin with assistive AI - document drafting, query support, or data review. The CDM implementations most likely to succeed are those that combine intelligent suggestions with strong human governance and expert CDM judgement.
7. Governance Model for Inspection-Safe AI Adoption
Scaling AI in CDM without compromising data integrity requires a governance model that satisfies ICH GCP E6(R2) principles. Every AI deployment should address the following pillars:
Context of Use
Define exactly what the AI is allowed to do. Scope must be documented: input type, output type, human review requirement, and applicable protocol or study scope.
Human Oversight
Require qualified review and approval for every AI output that influences clinical data, regulatory documents, or audit trail entries. Human judgement is not optional - it is the governance mechanism.
Validation and Testing
Test prompts, workflows, and outputs before use in live studies. Maintain validation logs, including failure modes and acceptable performance thresholds.
Audit Trail
Maintain complete documentation of AI interactions, citations, data sources, review decisions, and downstream actions. For FDA-regulated studies, AI tools that produce audit trail entries or influence electronic records fall under 21 CFR Part 11 (electronic records and electronic signatures) - ensure platforms meet Part 11 requirements for audit trail completeness, access controls, and system validation before deployment in a regulated study.
Data Privacy
Protect PHI. Use only approved environments for AI processing of clinical data. Ensure AI platforms meet applicable data governance and privacy requirements (ICH E6, GDPR, HIPAA where applicable).
SOPs and Training
Ensure all staff understand correct AI use, limitations, and escalation paths. Training must be documented and version-controlled alongside AI use cases.
The Operating Model
AI identifies. CDM verifies. System records. Human approves.
This model describes four roles, not a linear sequence - CDM professionals are engaged at every stage, not only at final approval. AI surfaces findings; CDM professionals verify clinical and operational appropriateness throughout the process; the system generates a complete audit trail in real time; and a qualified human formally approves any action that influences clinical data or regulatory documentation.
Final Perspective
AI should help CDM professionals work faster, sharper, and with more focus on judgment-dependent tasks. The implementations most likely to succeed are those with strong governance, defined accountability, and expert human judgement at the centre.
The goal is controlled augmentation - not uncontrolled automation.
About the Author
Neel Gajjar
CCDM®Clinical Data Manager II
Clinical Data Manager specialising in EDC systems, CDISC standards, and GCP-compliant data governance. Creator of the Clinical Research Learning Hub — a platform built to make rigorous clinical research education accessible to every professional in the field.
Connect on LinkedInAll content is expert-written and SME-reviewed. Regulatory references are verified against current ICH GCP E6(R2), FDA, and EMA guidance.
Comments
Leave a comment