
Introduction
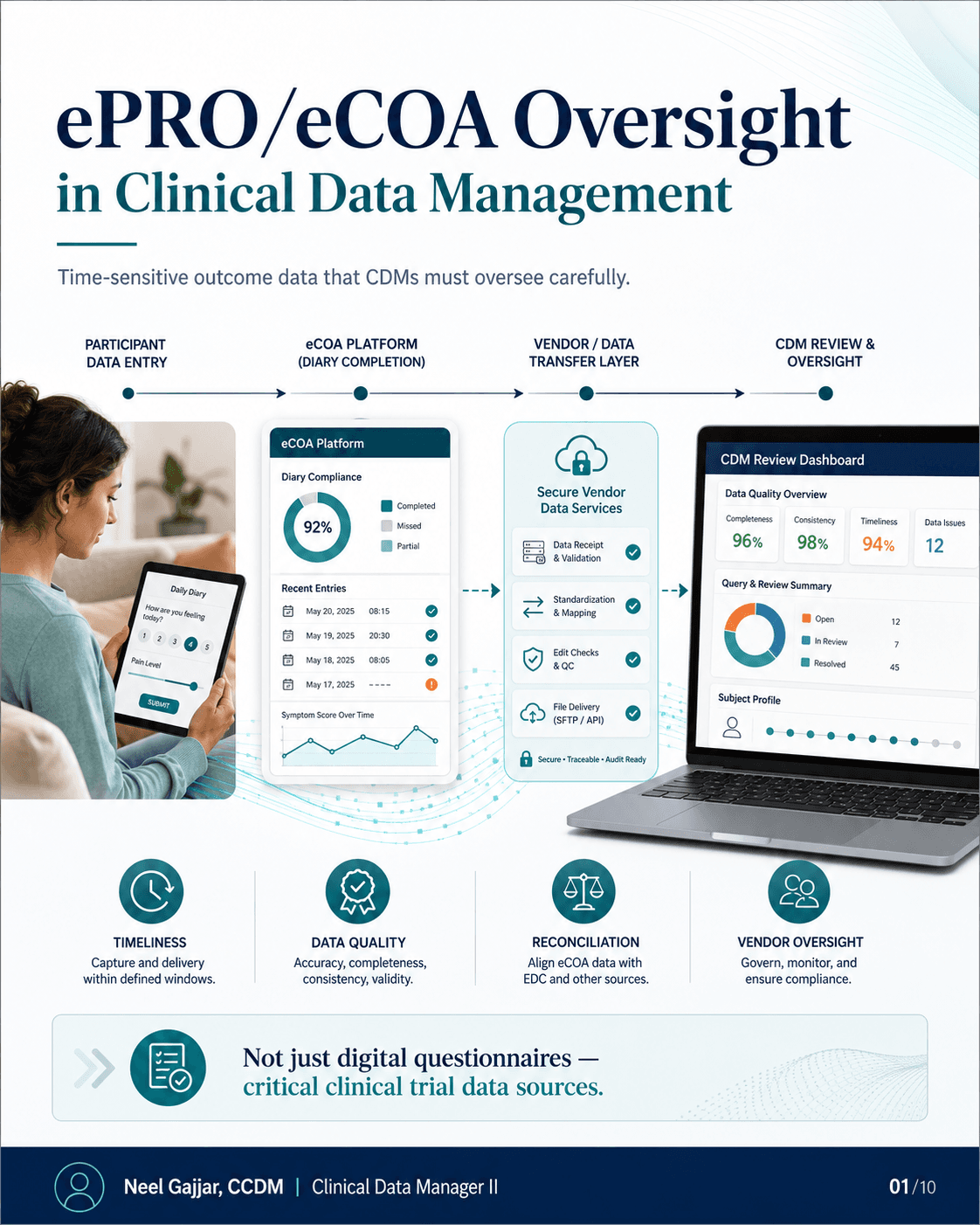
GDPR is not just a legal topic - for Clinical Data Managers, it is part of data quality, governance, and submission readiness. Privacy considerations affect daily CDM decisions across the entire study lifecycle: from which fields to include in an eCRF, to how vendor transfers are controlled, to how submission datasets are reviewed before transfer to a health authority.
Right Data. Right Way. Right Protection. Better Data Management. Better Participant Trust.
Why GDPR Matters to Clinical Data Managers
GDPR affects CDM decisions across five dimensions:
Protects participant personal data - Clinical trial data contains special category personal data under GDPR Article 9 (health data, genetic data, biometric data). The legal basis in clinical research is typically Article 9(2)(j) (scientific research) supported by national Member State law.
Supports trust and inspection readiness - Privacy documentation is part of the Trial Master File; documented controls strengthen regulatory inspection position
Controls access, transfer, and sharing - Role-based access, secure transfer mechanisms, and recipient list controls are CDM-operational responsibilities that GDPR requires to be documented
Reduces privacy and compliance risk - Unnecessary data collection, uncontrolled transfers, unmasked direct identifiers in submission files are compliance risks
Strengthens documentation and accountability - GDPR requires documented DPAs, lawful basis, and evidence of privacy controls - all of which CDM contributes to
Privacy by Design at Study Start-Up
Build GDPR controls before the first data point is collected. Privacy by design: right data, right purpose, right access, right evidence.
Protocol and ICF Review - Confirm purpose, data need, and privacy notice for every data element
eCRF and Database Design - Collect only required data; avoid direct identifiers; prefer Subject ID over personal identifiers
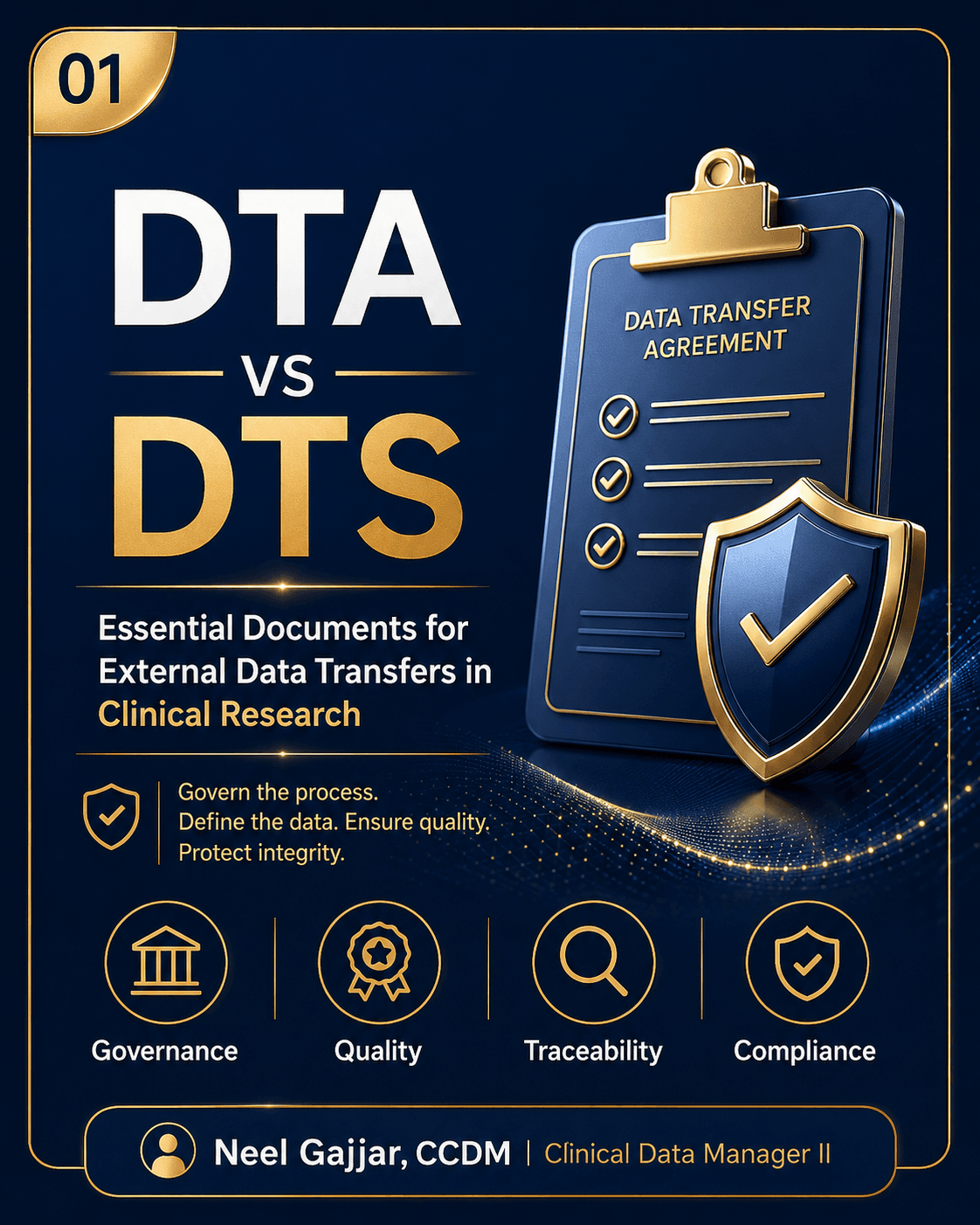
Vendor and Transfer Setup - Confirm DPA, DTA/DTS, secure transfer method, and recipient list for all vendors before first transfer
Access and Training - Use role-based access with documented access levels; maintain training evidence
QC and Documentation - Keep approvals, logs, and issue resolution evidence throughout the study
What CDM Owns vs What Sponsor/Legal/DPO Owns
CDM Owns / SupportsSponsor / Legal / DPO OwnsData minimisation in eCRF designLegal basis for processing (Article 6/9)Role-based access and user setupController vs processor classificationVendor file review and transfer controlsDPIA decision and privacy reviewFree-text review for identifiersCross-border transfer mechanism (SCCs)Pre-submission QC and documentationPrivacy notice and legal interpretation
CDM plays a critical operational role, but legal/privacy decisions must be confirmed by Sponsor, Legal, or DPO.
Data Minimisation in eCRF Design
Collect only what is necessary - nothing more. Before adding any field, ask:
Is it required by the protocol?
Is it needed for safety, eligibility, endpoint, or analysis?
Is it required for regulatory submission?
Can it be collected in a less identifiable form?
Can Subject ID be used instead of a direct identifier?
Avoid collecting unless justified: Full name, address, phone, email · Government ID or medical record number · Full date of birth when age or year is sufficient · Unnecessary personal details in free-text fields.
GDPR compliance does not mean removing required clinical data. It means collecting what is necessary, protecting it properly, and documenting the decision.
Pseudonymisation and Identifier Control
Clinical trial data is usually pseudonymised - not fully anonymised. If re-identification is possible, the data remains personal data under GDPR.
Use in clinical datasets: Subject ID · Screening ID · Randomisation ID · USUBJID · Site ID.
Do not routinely include: Full name · Phone number or email · Home address · Medical record number · Government ID.
CDMs must check datasets for inadvertent inclusion of direct identifiers - including in free-text fields - before any transfer or submission.
Vendor and Data Transfer Controls
Participant-level data should move only through controlled, approved pathways. For every external transfer:
Confirm DPA where required
Define DTA/DTS clearly before first transfer
Send only minimum necessary data
Use approved secure transfer methods (SFTP, encrypted portal - no unencrypted email)
Approve recipient list and access controls
Maintain transfer logs and reconciliation evidence
Do not transfer participant-level data until agreements, privacy roles, and secure transfer controls are confirmed.
DPIA and Privacy Escalation Triggers
CDM must know when to escalate to Sponsor, Legal, or DPO for a Data Protection Impact Assessment (DPIA). Escalate when:
Wearable or device data is collected
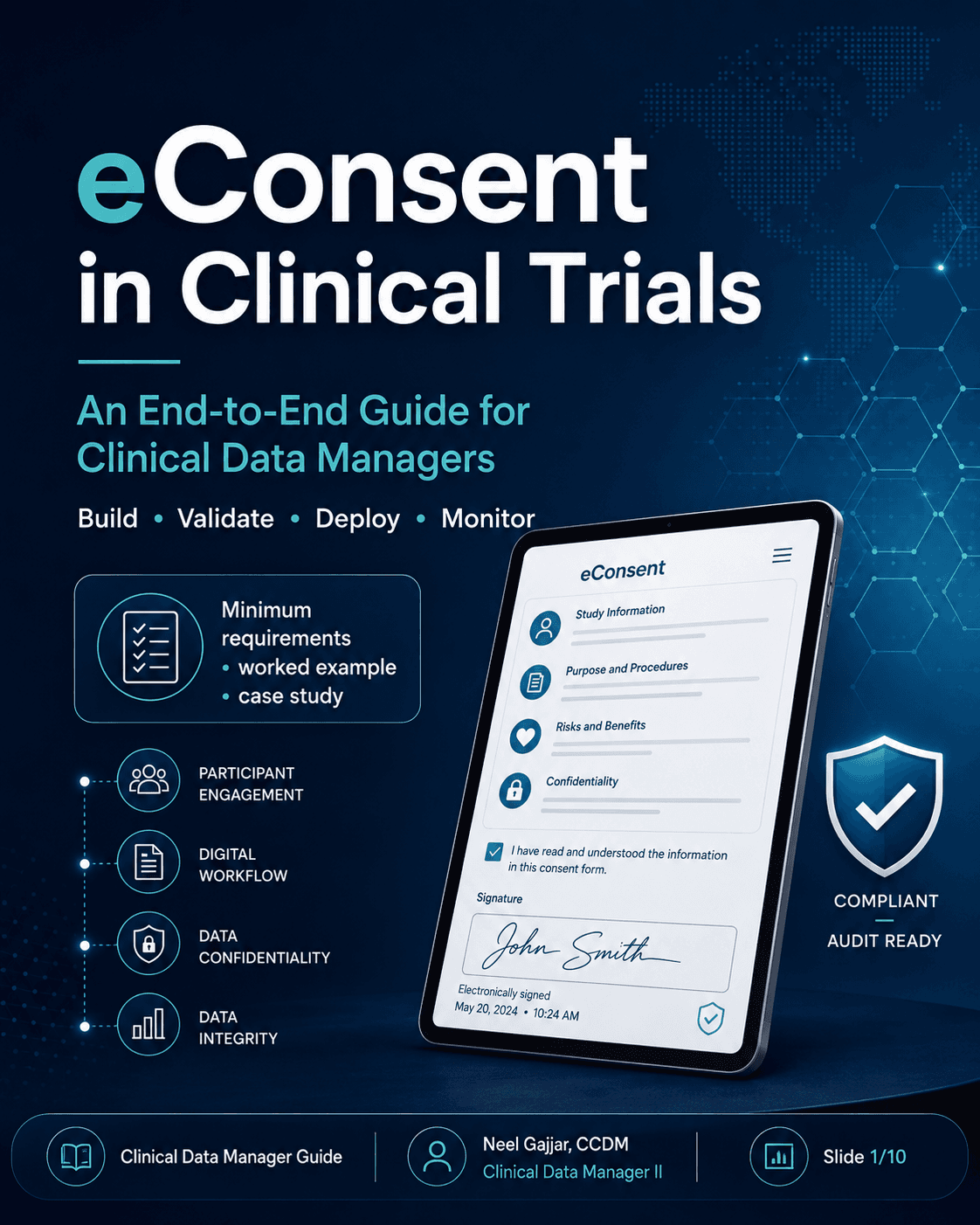
ePRO or eConsent platforms process participant data
Genetic or biomarker data is in scope
AI or machine learning analysis is used on participant data
Video, audio, or image data is collected or processed
Cross-border data transfer is planned
Direct identifiers will be accessible outside the site
A new vendor is added mid-study
A protocol amendment adds new data elements
Real participant data will be used in UAT or testing - using real participant data in non-production environments is one of the most frequently cited GDPR violations in clinical trial audits; use synthetic or anonymised test data for UAT wherever possible
Pre-Submission GDPR QC Checklist
Before transferring any dataset to a health authority:
Submission purpose confirmed
Recipient approved
DTA/DTS reviewed if applicable
DPA confirmed if applicable
Direct identifiers removed or justified
Free-text fields reviewed
Encryption key excluded
Required clinical data retained
Dataset QC completed
Secure transfer method confirmed
Cross-border transfer reviewed if applicable
Sponsor approval obtained
Transfer logged and final package filed/archived
Key Takeaways for Clinical Data Managers
GDPR should be built into the study from the start
CDM plays a critical operational role across the data lifecycle
Minimise, pseudonymise, secure, and document
Escalate privacy risks early - CDMs are often the first to identify DPIA triggers
GDPR does not mean removing required clinical data - it means protecting participant data while preserving scientific value
Privacy is part of data quality - and data quality must be defensible.
About the Author
Neel Gajjar
CCDM®Clinical Data Manager II
Clinical Data Manager specialising in EDC systems, CDISC standards, and GCP-compliant data governance. Creator of the Clinical Research Learning Hub — a platform built to make rigorous clinical research education accessible to every professional in the field.
Connect on LinkedInAll content is expert-written and SME-reviewed. Regulatory references are verified against current ICH GCP E6(R2), FDA, and EMA guidance.
Comments
Leave a comment