Introduction
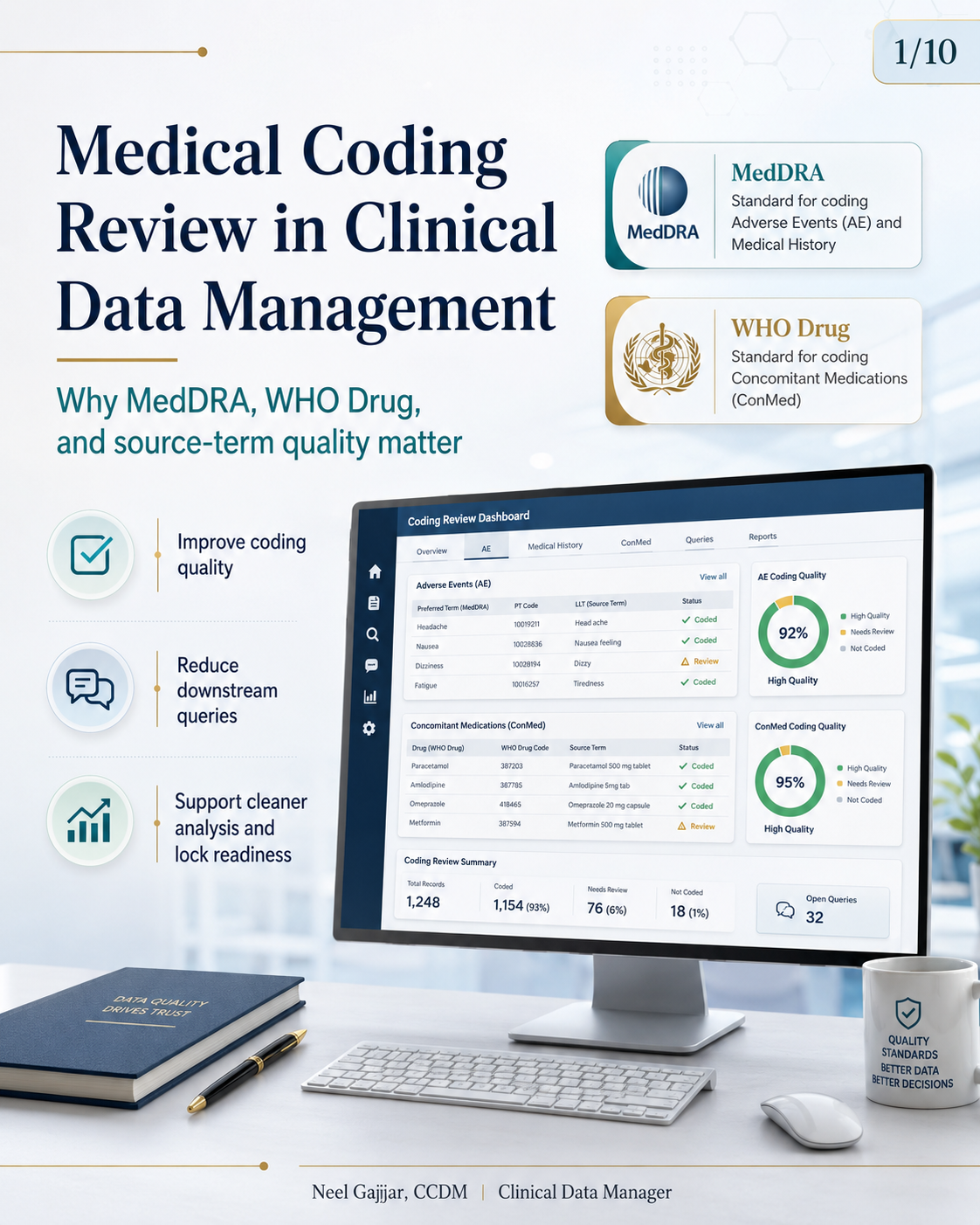
Medical coding in clinical trials is not a vendor output reviewed once at database lock. It is a data quality discipline that begins with how source terms are collected in the eCRF and ends with coded datasets that feed directly into safety analyses, regulatory submissions, and signal detection.
Medical coding quality is not only a vendor output. It is strengthened by good data collection, good review, and proactive CDM oversight.
Why Medical Coding Matters
Standardisation across sites and terms - Standard vocabularies ensure consistent coding across studies, sites, and reviewers
Better safety signal detection - Accurate coding informs consistent safety analysis; miscoded events can mask signals or create false aggregations
Cleaner tables, listings, and summaries - Coding errors appear directly in the clinical study report and submission datasets
Stronger medical review and reporting - Clear, consistent coding boosts review efficiency and confidence in conclusions
Better database lock readiness - Fewer coding issues mean less rework and a smoother lock
MedDRA vs WHO Drug: Two Dictionaries, Different Purposes
DictionaryUsed ForStructureMedDRAAdverse Events (AE), Medical History (MH)Hierarchical: SOC → HLGT → HLT → PT → LLT; supports safety analysis and regulatory reportingWHO DrugConcomitant Medications (ConMed)Supports medical product and drug name coding; standardises drug-related data
CDM practical view: Know which data goes to which dictionary · Review source-term quality before coding · Confirm coded outputs are complete and current before lock.
The MedDRA version must be agreed and documented in the DMP before the first coding run. Recoding after database lock due to a version upgrade is a significant and avoidable rework event. Most coding platforms run autocoding first (algorithmic matching), with manual review for non-matched terms - CDM should confirm both the match rate is reasonable and that manual review of all non-matched terms is complete.
What Source Data May Require Coding?
Adverse Events (AE) - Unfavourable medical occurrences (Headache, Nausea, Dizziness) - coded using MedDRA
Medical History (MH) - Pre-existing conditions or past diseases (Hypertension, Asthma, Migraine) - coded using MedDRA
Concomitant Medications (ConMed) - Medications taken during the study (Paracetamol 500 mg tablet, Metformin, Amlodipine) - coded using WHO Drug
Weak vs Strong Source Terms
Weak / UnclearStronger / ClearerPainHeadacheStomach issueNausea after doseBP medAmlodipine 5 mg tabletSugar drugMetformin 500 mg tablet
Better source terms: reduce coder ambiguity, reduce avoidable queries, and support more consistent analysis. CDM can improve source term quality through data entry instructions at build, targeted site training, and ongoing query review for recurring vague term patterns.
Common Coding Review Issues
Vague medical terms - Unclear terms lead to interpretation errors and wrong dictionary term selection
Incomplete medication names - Missing brand, generic, or qualifier information impacts accurate WHO Drug coding
Missing strength or formulation - Omitted strength or form leads to incorrect selection from multiple dictionary matches
Spelling variations and inconsistent wording - Typos and abbreviations cause autocoding mismatches requiring manual review
Uncoded or partially coded records - Incomplete coding increases discrepancy and review time
Late review close to database lock - Coding review left until the lock window is the leading cause of lock delays attributable to coding. Coding review should begin no later than 30% of planned enrolment.
CDM response: Review listings early · Query unclear source terms promptly · Confirm latest coded transfers are loaded before final review.
The CDM Role in Coding Review
Review coding listings and outputs - Examine coding summaries, uncoded lists, and quality metrics
Identify vague or uncoded source terms - Spot unclear, incomplete, or inconsistent terms needing attention
Query sites or data entry teams when needed - Clarify intent and obtain complete, standardised data upstream
Track trends and recurring issues - Monitor patterns to drive process and training improvements
Support coding readiness before lock - Ensure data is complete, consistent, and ready for final coding
CDM may not perform the coding directly, but strong CDM oversight improves coding quality.
Practical Coding Review Checklist
Confirm which forms/fields require coding
Confirm the correct dictionary is used (MedDRA for AE/MH, WHO Drug for ConMed)
Confirm current dictionary/version is in use and documented in DMP
Review coding status listings regularly
Check for uncoded or partially coded records
Query vague or incomplete source terms
Reconcile review outputs with study timelines
Confirm coding review is complete before lock
Coding Readiness Before Database Lock
Before database lock, CDMs should be able to answer six questions:
Are all AE, MH, and ConMed records coded or appropriately flagged?
Are unclear source terms queried - and responses received and reviewed?
Are recent coding outputs loaded and reviewed?
Are uncoded items explained or resolved with documented rationale?
Are study teams aligned on outstanding issues?
Is coding review complete enough for lock readiness?
Late coding review creates downstream risk for listings, analysis, and lock timelines.
Final Takeaway
MedDRA and WHO Drug serve different purposes - use the right dictionary for the right data
Clear source terms improve coding accuracy - better collection upstream reduces coder ambiguity and rework
Early review reduces downstream queries - proactive review during the study prevents lock-window bottlenecks
Coding readiness supports cleaner lock execution - stronger upfront quality means smoother database lock and audit readiness
Medical coding quality is not only a vendor output. It is strengthened by good data collection, good review, and proactive CDM oversight.
About the Author
Neel Gajjar
CCDM®Clinical Data Manager II
Clinical Data Manager specialising in EDC systems, CDISC standards, and GCP-compliant data governance. Creator of the Clinical Research Learning Hub — a platform built to make rigorous clinical research education accessible to every professional in the field.
Connect on LinkedInAll content is expert-written and SME-reviewed. Regulatory references are verified against current ICH GCP E6(R2), FDA, and EMA guidance.
Comments
Leave a comment